Value Based Payment (VBP) is a concept by which purchasers of health care (government, employers,…

What is a Special Needs Plans (SNP)?
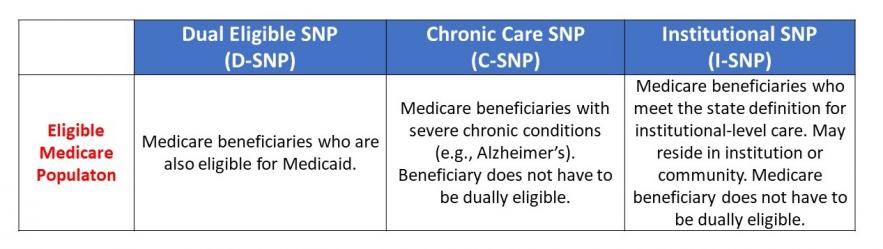
Special Needs Plans (SNPs) are a type of Medicare Advantage (MA) plan for individuals with special needs. This can mean an institutionalized individual (i.e., someone who lives in nursing home), a dually eligible individual (i.e., eligible for both Medicare and Medicaid), or an individual with a severe or disabling chronic condition.
The Medicare program pays SNPs on a capitated basis and requires that each have a Model of Care (MOC) approved by the National Committee for Quality Assurance (NCQA). The MOC provides the basic framework under which the SNP will meet the needs of each of its enrollees. There are three types of SNPs: Dual Eligible SNPs (D-SNPs), Chronic Care Special Needs Plans (C-SNPs), and Institutional Special Needs Plans (I-SNPs).
SNP types differ mainly in the populations they serve.
How many SNPs are there?

Are there provider-led SNPs?
Yes. Providers have long been selling Medicare Advantage plans, including SNPs. While there are a handful of systems and long-term care providers who own SNPs, there are many providers who partner with larger plans (e.g., Optum) to offer plans to their patients and residents.
Why are providers creating SNPs?
Many providers see taking on health care risk – through participating in value-based care demonstrations such as bundled payment or by forming accountable care organizations or health plans — as the only option for gaining control over their financial future and capturing the return on their investments in improved patient outcomes.
How are I-SNPs unique?
Facility settings can support effective care management, and I-SNPs can reward providers for the avoidance of resident hospitalizations.
I-SNPs originated from a demonstration of the Evercare model, in which onsite nurse practitioners in nursing homes deliver care aimed at reducing unnecessary hospitalizations. While providers can and do operate D-SNPs and C-SNPs on a smaller scale, these plans must be offered to community-dwelling individuals. The provider-owned I-SNP, on the other hand, gives providers direct Medicare funding through the premium to finance onsite primary care and care coordination for the long-stay resident population.
Facility operators have the ability to observe a complex care population in their home environment and to manage health care for many high-need individuals in one location.
How many provider-led I-SNPs exist and are they increasing in popularity?
There are 44 provider-led I-SNPs (as of June 2019), with 17,749 enrollees. Yes, the number of provider-led I-SNPs has been increasing steadily.

Are SNPs here to stay?
Yes. In 2003, Congress authorized SNPs to market to special populations. SNPs were first offered in 2006. Authority for SNPs was extended in various laws, including the Affordable Care Act. On February 9, 2018, President Trump signed the Bipartisan Budget Act of 2018, which included the CHRONIC Care Act, which permanently authorized SNPs.
Related Posts